
The field of multiplex tissue imaging has been growing quickly over the last few years with a focus on preclinical applications, which leads to the logical question of “when will multiplex tissue imaging start to be used in the clinical space?” As a company, Visikol began its journey developing tissue clearing reagents and kits that were originally planned to be used as a clinical tool to improve the diagnosis of cancer and the outcomes for patients. While these tools provide the ability to capture more data from tissues and to provide a higher level of sensitivity compared to human driven pathology for many applications, the interesting thing is that they tend not to actually improve patient outcomes. The reason for this is that if for a given disease there are only two options (e.g., treat with a therapeutic, don’t treat with a therapeutic) and the decision is based on a binary decision point (e.g., presence of a marker), then providing more sensitivity and “better” data will only confer an impact if there is a large degree of false negatives, which there are typically not. Further, if the new approach is more expensive, on the whole the introduction of the approach might be worse for patient outcomes and overall healthcare costs.
The key learning from this is that a more sensitive and advanced approach for diagnosis and tissue characterization is only useful if it changes the clinical outcome for the patients. If there is only one treatment or a few treatment paradigms that are easily stratified from one another today, then an advanced approach will offer little value and will not be adopted, even though it is new and more sensitive, accurate, robust etc.
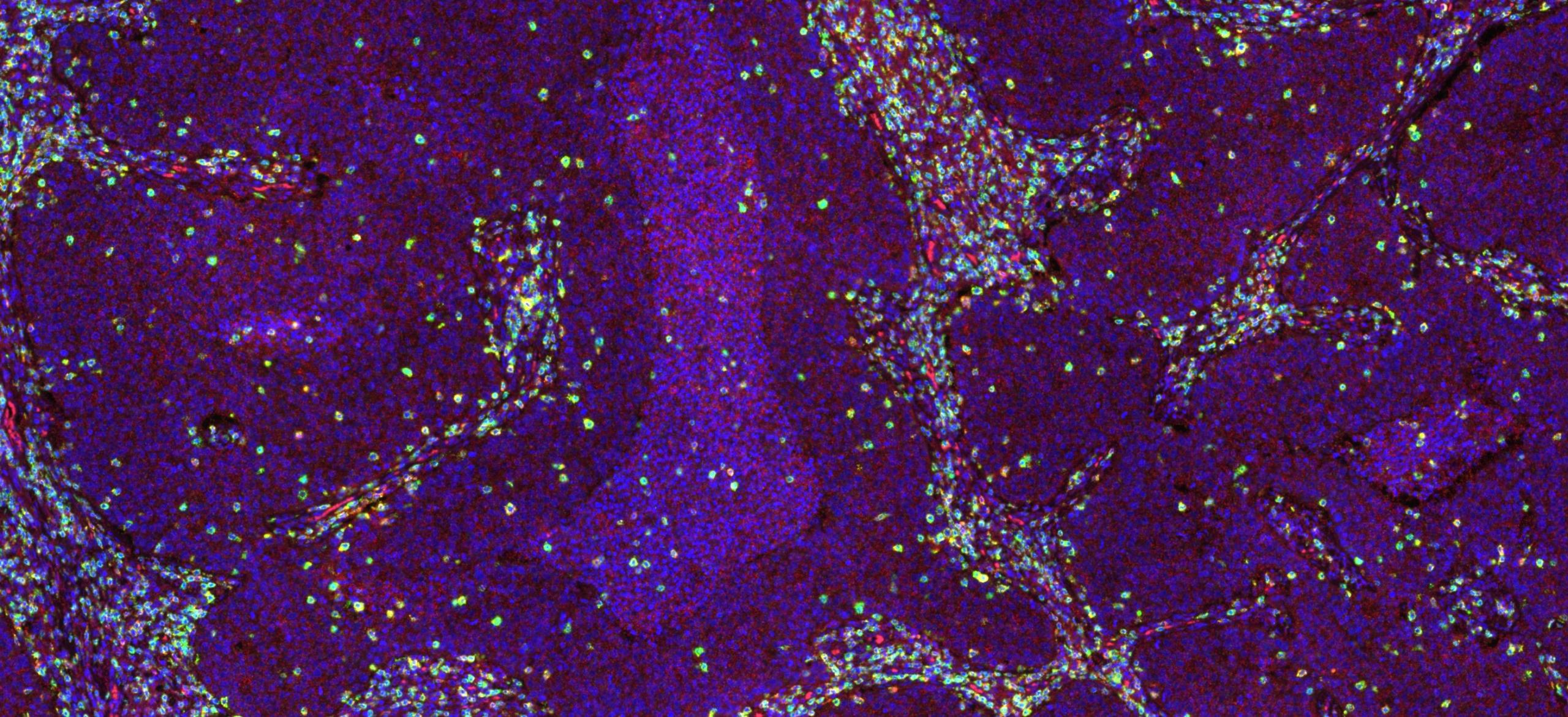
When thinking of multiplex tissue imaging and evaluating a biopsy with a technique capable of generate terabytes of imaging data from a single slide, the technique will only be helpful if that information can be actionable. The main business case for this insight is in the use of immuno-oncology therapeutics where each treatment is highly specific to the individual patient and their disease. In this new paradigm, the efficacy of a therapeutic will be based on the individual and not on highly broad categorizations. This means that the introduction of many immunotherapies will not only allow for the introduction of more advanced characterization tools, but the very nature of these therapeutics will demand for it.
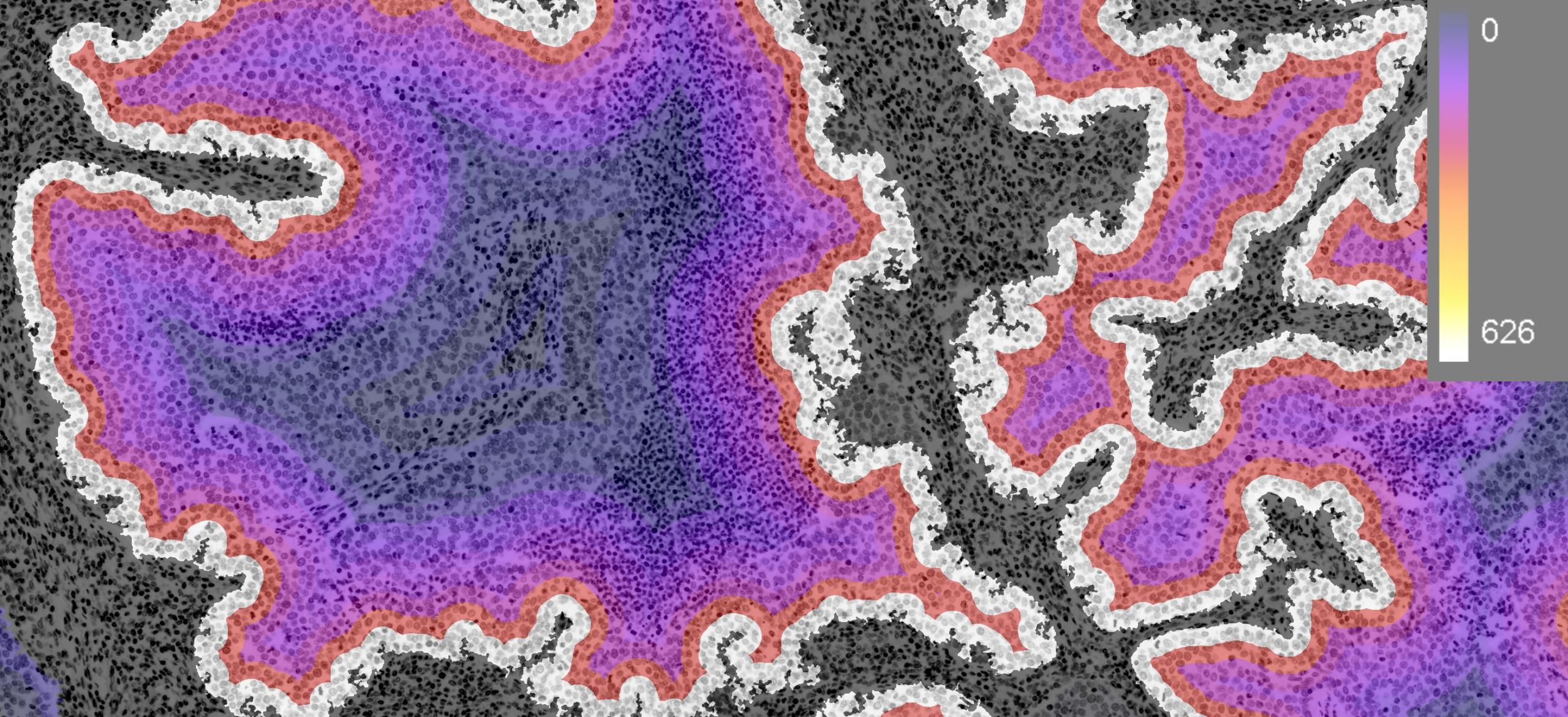
Heatmap of lung cancer tissue section depicting number of CD3+ cells as a function of distance into the tumor.
Therefore, advanced tissue characterization approaches will only start to be readily adopted in lock-step with more advanced and individualized treatment approaches, whereas a complex array of factors will decide if a patient is amenable to one treatment or another. For example, the distance T-Cells infiltrate into a tumor might be a unique biomarker for a novel treatment which is a characterization endpoint only possible through the use of advanced multiplex tissue imaging approaches.

As a company, we see this shift already starting, as pharmaceutical companies are beginning to add multiplex tissue imaging data to their clinical trials to ascertain more information about the patients and to stratify patients. As more robust correlations of therapeutic efficacy and multiplex endpoints come out of clinical trials, these tools will start to be more engrained into the overall clinical tissue imaging workflow. However, to make this jump they will need to demonstrate that they confer real financial and also patient outcome benefits.
Interested in learning more about using multiplex tissue imaging for your project? Contact us today!